


INTRODUCTION
Insomnia is characterized by subjective complaints of difficulty initiating or maintaining sleep and/or experiencing non-restorative sleep. Due to such sleep problems, insomnia patients also frequently complain of daytime impairments across various dimensions, including occupational, academic, and/or social situations [1-3]. In fact, daytime dysfunction is included as an essential item in the diagnostic criteria for insomnia. Although daytime dysfunction is highly correlated with insomnia disorder, understanding regarding the mechanisms underlying this relationship is lacking, and previous studies have not produced consistent results.
To date, most studies of cognition in insomnia patients have focused on attention, memory, and executive function. For example, a recent meta-analysis [4] found that insomnia patients exhibited decreases in perceptual processes, alertness, complex attention, retention, working memory, episodic memory, and problem solving but not in verbal functions, information processing, selective attention, divided attention (DA), sustained attention (SA), procedural memory, verbal fluency, or cognitive flexibility. Although insomnia generally appears to have negative effects on cognitive functioning, the findings of this meta-analysis suggest that previous studies investigating this issue have not found consistent results, even within a single cognitive domain. Furthermore, although the effects of sleep deprivation on cognitive function have been studied for many years, this literature also includes inconsistent findings. For example, in contrast to the expectation that sleep deprivation causes cognitive dysfunction, many findings have been negative. One possible theoretical explanation for these negative results is the lapse hypothesis [5], which proposes that sleep loss does not completely damage cognitive function but rather results in moment-to-moment variability in performance due to an unstable awake state. Thus, between lapses of attention, people who experience sleep loss may function as well as they typically would. Accordingly, attention may be a core element underlying daily dysfunction in insomnia patients.
SA is the ability to maintain focus for long periods of time in complex circumstances while experiencing interference. This type of attention is a fundamental aspect of various daily human activities, such as cooking, reading books, and listening to lectures, and is required by almost all people. Previous studies of SA in insomnia patients typically required participants to pay attention for approximately 10 min. The second type of attention, DA, which involves the ability to simultaneously process two or more elements, is important when multitasking, such as talking while driving; thus, it exacts a higher cognitive processing burden. Some studies have revealed significant impairments in the attention performance of insomnia patients, including slower reaction times (RTs) or lower levels of accuracy, whereas others have not [6-9].
Due to these discrepancies regarding attention performance in insomnia patients, it is important to improve the current understanding of this issue by considering the unique maladaptive thoughts of insomnia patients. Patients with chronic insomnia frequently report misperceptions about sleep [10,11], which is one factor by which bad sleep habits are created. For example, insomnia patients might choose to have a less demanding day, which may include skipping exercise or scheduling a nap to compensate for their sleep loss, which can lead to repeatedly disrupted sleep cycles [12]. Insomnia patients also experience excessive worry about sleep and tend to catastrophize the results of sleep loss, which increases the likelihood of a negative mood [13]. Additionally, an epidemiological study of a community-based sample revealed that people with insomnia were 9.82 times more likely to have significant depression and 17.35 times more likely to have anxiety than people without insomnia, even after controlling for confounding factors such as ethnicity and sex [14]. Therefore, the present study investigated how the negative emotional states or maladaptive beliefs of insomnia patients would affect attention.
The present study compared the attention performance of insomnia patients with that of healthy controls to investigate correlations between attention performance and characteristics of insomnia patients, including negative mood, catastrophic worries about sleep, and maladaptive beliefs. It was hypothesized that attention dysfunction in insomnia patients would vary depending on the specific clinical symptoms.
METHODS
Participants
All participants were recruited via advertisements at Seoul National University Hospital and completed the study requirements voluntarily. The present study included 66 participants who were enrolled from two different sleep-related studies that employed identical procedures for the administrations of questionnaires, computerized attention tasks, and nocturnal polysomnography (nPSG) tests. All participants with insomnia met the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) [15] criteria for chronic insomnia. Patients diagnosed with serious neurological or psychiatric disorders following psychiatric interviews during the enrollment period were excluded from the study. All participants completed a one-night nPSG (Profusion PSG3; Compumedics; Abbotsford, VIC, Australia) assessment in a sleep laboratory to evaluate objective sleep characteristics and to rule out other sleep disorders such as sleep apnea or periodic limb movement disorder.
A total of 10 participants were excluded due to missing questionnaire data (2 participants), missing nPSG data (1 participant), the presence of a sleep disorder based on nPSG results [1 participant had an Apnea–Hypopnea Index (AHI) >15, and 3 had a Periodic Limb Movements Index (PLMI) >15], or a score of zero on the SA task (3 participants). Ultimately, 30 patients with insomnia disorder (INS; 24 females and 6 males, mean age: 43.87±13.73 years) and 26 healthy controls (HC; 13 females and 13 males, mean age: 37.08±13.40 years) were included in the final analyses. The study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. 1603-073-748, 1806-174-955).
Computerized attention task
SA and DA were measured using the computerized comprehensive attention task (CAT), which has subsets of tasks that evaluate comprehensive attention and working memory functions. The CAT has been standardized for children and adolescents [16] as well as adults [17].
The SA task assesses the ability to maintain attention under long and repetitious circumstances. Participants are instructed to press a button for every visual stimulus (various shapes presented every 2 s) but not for stimuli of a specific shape (‘X’ shape), which are the targets. The task persists for 10 min and participants are required to maintain focus during the long series of presentations to be able to successfully inhibit their responses to the target stimuli. The number of commission errors (CE), number of omission errors (OE), and RT are recorded as behavioral data.
The DA task assesses the ability to simultaneously process multiple demands. This test is a dual one-back task in which two independent sequences are simultaneously presented with visual and auditory stimuli, and participants are required to divide their attention to receive and process two different types of information sources at the same time. Stimuli are presented every 2 s for 3 min. CE, OE, and RT are recorded as behavioral data.
Questionnaires
All participants completed several sleep-related questionnaires, including the Epworth Sleepiness Scales (ESS), the Pittsburgh Sleep Quality Index (PSQI), the Dysfunctional Beliefs and Attitudes about Sleep Scale 16 (DBAS-16), and the Insomnia Severity Index (ISI), as well as the Beck Depression Inventory (BDI) and the Beck Anxiety Inventory (BAI). The PSQI assesses sleep quality in terms of sleep latency (SL), sleep duration, sleep disturbance, and daytime dysfunction over a 1-month period; the DBAS-16 is an abbreviated version of the DBAS and assesses sleep-related beliefs; the ESS assesses daytime sleepiness; and the ISI assesses the degrees of problems in initiating sleep, maintaining sleep or experiencing early awakening, and distress caused by the sleep problem. The HC subjects also completed the ISI questionnaire. The BDI assesses the intensity of depressive symptoms, and the BAI assesses the intensity of anxiety symptoms over the past week.
Statistical analysis
All behavioral data were automatically calculated by the computerized task program; CE, OE, and mean RT were recorded. First, group differences were analyzed with multivariate analysis of variance tests, which was performed four times for each categorized variable, i.e., the behavioral results of the SA task, behavioral results of the DA task, questionnaire scores, and nPSG results. Age and gender were included as covariates.
Second, partial correlations between cognitive performance measures (SA and DA tasks, separately) and various individual variables (questionnaire scores and nPSG) were performed after controlling for age and gender. Because the only difference between the groups was a trend toward a significant difference in the mean RT, only RT was used to perform correlation analyses with the other data (i.e., the questionnaires and nPSG). The correlation analyses on each group were performed separately, and all data were analyzed using PASW Statistics for Windows (Version 18.0; SPSS, Inc., Chicago, IL, USA). p-values <0.05 were considered to indicate statistical significance.
RESULTS
Group comparisons
Both attention tasks showed trends for significant differences between the two groups in mean RT [SA task: F(1,54)=3.62, p=0.06; DA task: F(1,54)=3.80, p=0.06] (Table 1), with the INS group having longer RTs than the HC group on both the SA and DA tasks. The INS group also had significantly higher scores on the ISI, PSQI, DBAS, BDI, and BAI (all p<0.05) (Table 1). However, there were no significant differences in ESS scores or nPSG measurements (Table 1).
Correlations with cognitive performance
Questionnaires
ESS. There were no significant correlations between the mean RT and ESS score in either group for either attention task.
PSQI. There were no significant correlations between PSQI score and mean RT on either attention task in either group. However, trends toward significance were found in the HC group for the associations of mean RT with both attention tasks and with the PSQI score (SA task: r=-0.37, p=0.07, DA task: r= -0.38, p=0.07) (Table 2). Subsequent correlation analyses assessing the sub-components of the PSQI questionnaire revealed a significant negative correlation between the mean RT on the DA task and PSQI component number 1 (subjective sleep quality; a higher score is indicative of worse quality) in the HC group (r=-0.46, p<0.05) (Fig. 1A).
DBAS-16. There were no significant correlations between the mean RT and DBAS score in either group or on either attention task.
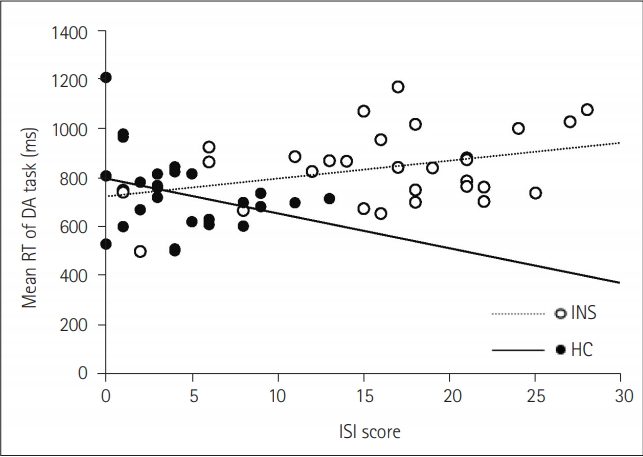
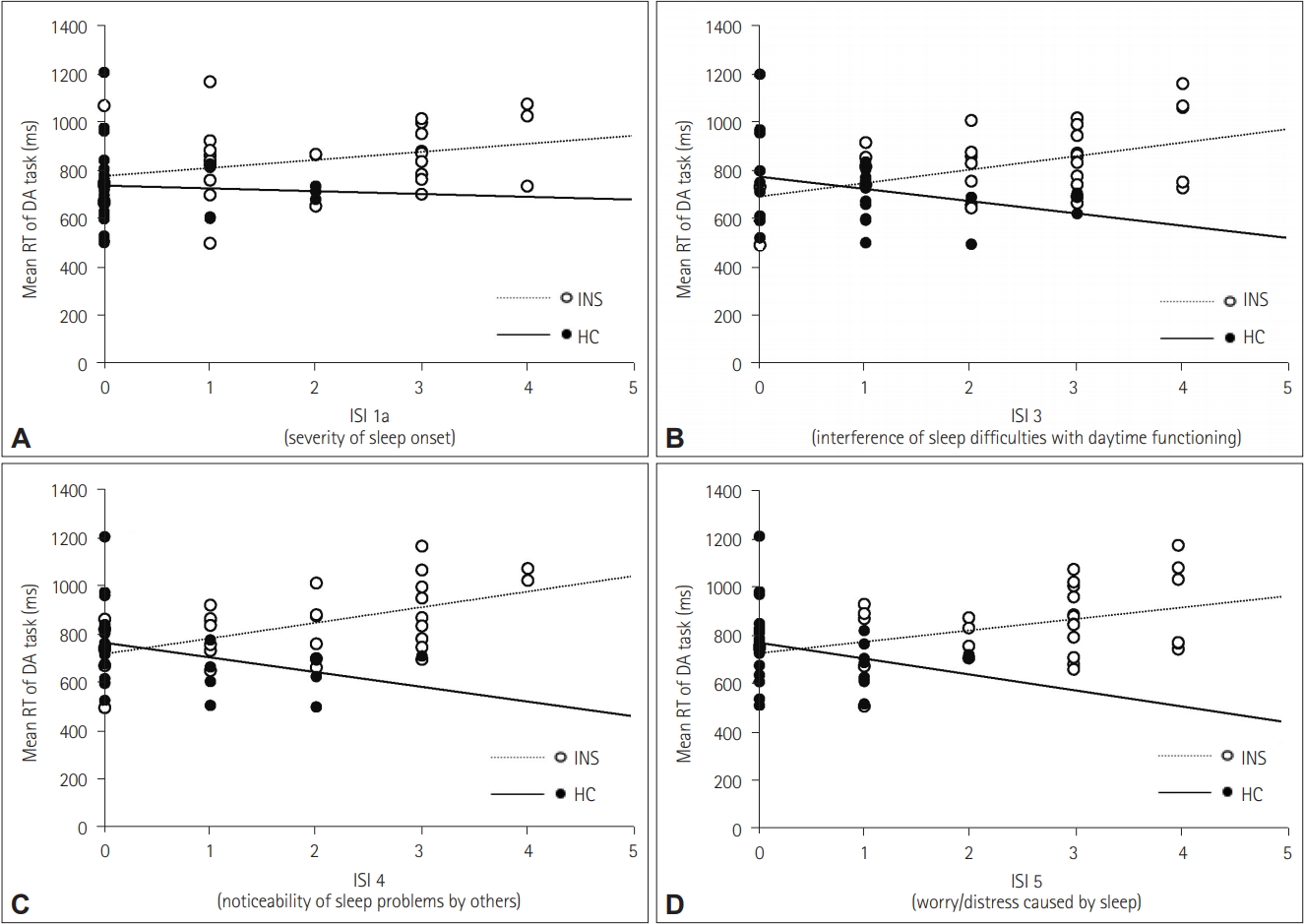
ISI. The two groups exhibited opposite correlation patterns, particularly for the mean RT on the DA task. The INS group showed a positive correlation between ISI score and mean RT on the DA task (r=0.40, p<0.05), whereas the HC group showed a negative correlation (r=-0.58, p<0.05) (Table 2, Fig. 2). In subsequent correlation analyses of the sub-items of the ISI questionnaire, the INS group showed a trend toward a positive correlation for all items and significant results for items 1a (severity of sleep onset), 3 (interference of sleep difficulties in daytime functioning), 4 (noticeability of sleep problems by others), and 5 (worry/distress caused by sleep) (Fig. 3). The HC group showed a trend toward a negative correlation for all items and significant results for items 3 and 5 (Fig. 3). There were no significant correlations between mean RT on the SA task and ISI score in either group.
BDI. There were no significant correlations between mean RT and BDI score in either group or for either attention task.
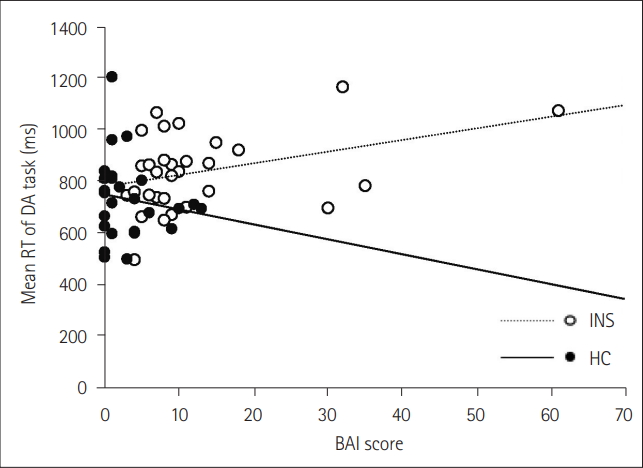
BAI. The INS group showed a positive correlation between mean RT on the DA task and BAI score (r=0.39, p<0.05) (Table 2, Fig. 4). The HC group showed a trend toward a negative correlation (r=-0.28, p=0.19). There were no significant correlations between mean RT on the SA task and BAI score in either group.
nPSG. Results showed several significant correlations between attention performance and the nPSG data (Table 2). In the HC group, the mean RT on the SA task was significantly correlated with sleep efficiency (SE) (r=0.42, p<0.05) (Fig. 1B), and the mean RT on the DA task was significantly correlated with % of NREM stage 3 (r=0.58, p<0.05). In the INS group, mean RT on the DA task was significantly correlated with % of REM (r=0.39, p<0.05) and SL (r=0.44, p<0.05).
DISCUSSION
The present study aimed to determine whether insomnia patients would differ in attentional function compared with healthy controls and to examine the relationships of these differences with the specific characteristics of insomnia. Although negative emotions and maladaptive thoughts are associated with sleep issues, there were no significant differences in attention performance between the INS and HC groups in the present study, consistent with previous findings [3,4]. However, there were several trends toward significant differences (p=0.06). Interestingly, sleep-related symptoms had opposite effects on attention performance in the two groups. Overall, when insomnia patients experienced sleep disturbances or had negative expectations related to sleep loss, their attention performance suffered in a severitydependent manner, with performance becoming poorer as the severity of sleep issues increased. Conversely, when the control group experienced sleep disturbances or had negative effects related to sleep disturbances, they exhibited improved attention performance.
In terms of the specific sleep measures, a high ISI score was associated with poor attention performance in the insomnia patients, particularly with sub-items related to their maladaptive beliefs, including noticeability of sleep problems by others, worry/ distress caused by sleep, and interference of sleep difficulties in daytime functioning. The HC group showed opposite results, which is not surprising. The maladaptive beliefs of insomnia patients are a major factor leading to chronic insomnia, as these beliefs intensify arousal levels to sleep-related stimuli and prompt safety behaviors that generate bad sleep habits, ultimately resulting in repeated disturbance of sleep during the night and dysfunction during the day [10]. This subjective misunderstanding of sleep occurs even when their sleep is not objectively disturbed [18]. This psychological process seems to affect the mindset necessary to maintain attentional effort for functioning well in daily life [19]. The present results confirm that these maladaptive beliefs have a negative effect on maintaining stable attentional efforts.
Of the ISI sub-items assessing various types of sleep disturbance, poor attention performance was related to sleep initiation difficulty in the INS group. Insomnia patients frequently report uncontrolled and unwanted worries or thoughts about sleep in the presleep stage [20,21]. These unconstructive worries and ruminations result in psychological and physiological arousal and delay sleep onset [22,23], this arousal state is strongly associated with severe anxiety in insomnia patients [10]. Relatedly, insomnia patients’ anxiety scores were correlated with poor attention performance. Unlike other cognitive domains, attentional effort requires heightened and active psychological effort and is thus vulnerable to characteristics exhibited by insomnia patients, including repetitive sleep-related stress and heightened anxiety levels.
In contrast, poor sleep quality (based on PSQI scores) was associated with good attention performance in the HC group, and a similar result was observed regarding SE (as measured by nPSG). Many previous studies of sleep deprivation have reported that sleep loss does not affect attention performance and have further suggested that these negative findings may be due to the compensatory recruitment of cognitive engagement following sleep deprivation. For example, one model suggests that sleep deprivation may have a more significant effect on simple or monotonous tasks that require less high-level top-down control relative to complex tasks [24]. Moreover, attention performance is impaired when the task load is increased beyond one’s ability to compensate, such as during a triple task compared with a dual task [25], a commonly used paradigm in sleep deprivation studies. However, the present study found that a greater degree of sleep disturbance resulted in better attention performance in the HC group; this may be due to motivation levels. Motivation is required for the maintenance of attentional efforts; it was previously explained as a cognitive incentive for optimizing input processing, detecting errors, and focusing processing resources under challenging circumstances [26]. As mentioned above, following sleep disturbance, attention performance is more vulnerable during tedious and repetitive attention tasks than during complex tasks that require high levels of top-down control. The task used in the present study seems to have triggered sufficient top-down control, and it may be that, in the presence of increased sleep disturbance, highly motivated cognitive engagement was required of the HC group to enable compensatory resources.
The present study has several limitations that should be considered. First, it was not possible to directly compare the cognitive properties of SA with those of DA. In the HC group, severe sleep disturbances were associated with better performance on both the SA and DA tasks, whereas associations between attention performance and the clinical characteristics of insomnia patients were observed only for the DA task. This finding differs from those of previous studies, which reported that sleep loss was more relevant during simple than during complex attention tasks. Perhaps the 10-min SA task in the present study was at high enough level that insomnia patients were not affected by their clinical symptoms. However, this possibility is only a hypothesis because it was not possible to directly compare performance on the SA task with that on the DA task or to determine why this difference occurred. In the future, it would be valuable to investigate how differing levels of attention might be related to the symptoms of insomnia patients.
Based on the theoretical lapse hypothesis of sleep deprivation, which suggests that sleep deprivation does not completely impair cognitive function but rather aggravates attention dysfunction as a result of an unstable awake state [5], the present study examined attention performance to better understand the daily dysfunction of insomnia patients. The results showed that sleep-related difficulties, such as a lower quality of sleep or worries/distress about sleep, had a positive influence on attention function in the HC group, which likely occurred because these issues motivated them to use compensatory resources. On the other hand, these difficulties had a negative impact on insomnia patients and resulted in poorer attention. These results indicate that the attention complaints of insomnia patients may be associated with a failure to maintain attentional efforts due to sleep-related psychological symptoms or anxiety rather than due to objective cognitive impairments.