Differential Profiles of Cortisol, Components of Autonomic Nervous System, and Self-Rated Health in Premature Ventricular Contraction: An Observational Study of Three Circadian Types
Article information

Abstract
Objective
Premature ventricular contraction (PVC) exhibits one of the three circadian patterns, namely fast-type, slow-type, and independent-type. This study aimed to investigate whether the cortisol-marker of hypothalamic-pituitary-adrenal axis, autonomic nervous system activity, and perceptive self-rated health are associated with the three PVC circadian types.
Methods
This cross-sectional observational study recruited 65 idiopathic PVC subjects (23 fast-, 20 slow-, and 22 independent-type) as well as 5 control subjects. Each subject underwent a 24- hour Holter to examine PVC burden and heart rate variability, collected saliva for cortisol and norepinephrine level measurement at 6–7 am, 10–11 am, and 10–11 pm, and recorded their self-rated health scales. Furthermore, univariate and multiple linear regression were conducted to investigate the associations between the independent variables and PVC burden.
Results
The average PVC burden was 15.7%, 8.5%, and 13.6% in fast-, slow-, and independent-type idiopathic PVCs, respectively. Multiple linear regression showed that the high burden of fast-type idiopathic PVC was associated with higher cortisol levels and lower parasympathetic nervous system tone. The high burden of slow-type idiopathic PVC was associated with lower cortisol levels and lower sympathetic nervous system tone. Meanwhile, in independent-type idiopathic PVC, the high burden was associated with higher cortisol levels and sympathetic nervous system tone as well as lower self-rated health scales.
Conclusion
Each PVC circadian type is uniquely related to hypothalamic-pituitary-adrenal axis, autonomic nervous system, and selfrated health. Assessment of PVC circadian type needs to be carried out routinely considering the differences in the underlying associated factors.
INTRODUCTION
Idiopathic premature ventricular contraction (PVC) is the most common type of ventricular arrhythmia with a prevalence of 5%–12% [1]. Recent data shows that there are three PVC burden circadian patterns, classified as fast-type (48% of cases), slow-type (16% of cases), and independent-type (36% of cases) [2]. In fasttype, the PVC burden is positively correlated with heart rate. Fasttype PVC burden increases as the heart rate increases which leads to high PVC burden during daytime and low PVC burden during nighttime. Conversely in slow-type, the PVC burden is negatively correlated with heart rate. Slow-type PVC burden increases as the heart rate decreases, hence PVC burden rises overnight to early morning. In independent-type, the PVC burden stays consistent throughout day and night regardless of increase or decrease in heart rate [3].
Nearly all of the temporal cycles of human life are governed by input from the main circadian clock located in the suprachiasmatic nucleus (SCN) [4]. SCN stimulates circadian rhythms of peripheral clocks including the heart through neural and humoral mechanisms, by the activities of the autonomic nervous system (ANS) and the release of cortisol and melatonin rhythmically through hypothalamic-pituitary-adrenal (HPA) axis [5]. To our knowledge, there are no previous studies describing the variations in activation of HPA-axis and ANS as well as their association with PVC burden. Furthermore, identifying the HPA-axis and ANS circadian rhythm of each PVC circadian type would be of value for understanding and modifying time of day of PVC treatment and thereby potentially improving patient outcomes.
This study also focused on the association between PVC burden circadian types with stress and self-rated health. Self-rated health is a commonly used metric of overall health, and it has been applied in diverse populations, including Indonesia [6]. Prior research provided empirical evidence that ventricular arrhythmias were associated with perceived stress and depression [7,8]. Studies have additionally found stress to have significant impact on cardiac arrhythmogenesis, alteration in catecholamine release, and significant effect on atrial and ventricular electrical indices [9,10].
We performed this observational study to compare circadian rhythms of cortisol, norepinephrine, ANS, stress and self-rated health in PVCs of different circadian types. We also sought to identify and describe their associations with PVC burden. Our main question was: to what extent do fast-, slow-, and independent-type PVC differ in the HPA-axis, ANS, and psychological aspects? Furthermore, we wanted to find out what parameters are associated with the three PVC circadian types.
METHODS
Study population
This cross-sectional observational study was formally approved by the Ethical Committee of National Cardiovascular Center Harapan Kita, Indonesia (Ethical Clearance no. UM.01.05/2.2.2/209/2022). Written informed consent was obtained from all participants. In the a priori sample size calculation, we previously estimated that at least 60 subjects (20 per group) were required to detect a mean absolute difference of approximately 50% for the expected changes in HRV, salivary cortisol and/or norepinephrine concentrations between the morning, day, and evening as well as between the three circadian types of idiopathic PVC with an α of 0.05, a β of 0.2, and a statistical power of 80%.
From June 2022 to December 2022, we consecutively recruited idiopathic PVC patients attending the outpatient clinic of the National Cardiovascular Center Harapan Kita Jakarta, Pakuhaji General Hospital Tangerang, and Bun Hospital Tangerang. Patients with PVC burden equal to or greater than 5% per day during 24-hour Holter recording were identified and the circadian rhythm pattern was then determined as fast-type, slow-type, or independent-type PVC. If PVC burden was positively correlated with heart rate (Pearson’s correlation coefficient ≥0.3 with p<0.05), then the patient was classified as fast-type PVC. If PVC burden was negatively correlated with heart rate (Pearson’s correlation coefficient ≤-0.3 with p<0.05), then the patient was classified as slow-type PVC. If there is no relationship between PVC burden and heart rate (Pearson’s correlation coefficient -0.3 to +0.3), then the patient was classified as independent-type PVC. Due to the higher prevalence of fast- and independent-type PVC, their sample sizes were fulfilled earlier than slow-type PVC. After that, we pursued recruiting slow-type PVC until we reached 20 eligible subjects.
Clinical data of each subject were collected from medical interviews and questionnaires. Demographic and anthropometric characteristics included age, gender, body mass index (BMI), previous medical history, and current medication usage. Patients with any form of structural heart disease (ejection fraction below 50% or regional wall motion abnormalities on echocardiographic examination, moderate to severe heart valve disorders, and congenital heart disease), multifocal PVCs, atrial fibrillation, pulmonary hypertension, impaired liver or renal function, electrolyte abnormalities, and home address outside of Jakarta and Tangerang were excluded from the study. None of the study participants had high-stress level (Self-Reporting Questionnaire 20 ≥8) or extreme times of waking or sleeping and eating (i.e., bedtime <22:00 or >00:00 [>2 days a week] and/or waking time <04:00 or >09:00), nor had they worked at night shift in the last 2 years that could have influenced cortisol or norepinephrine production. In addition, five healthy adults who were matched for age and gender were enrolled as controls. These controls were recruited from well-patient visits in the clinic.
Holter examination protocol
The 24-h electrocardiogram (ECG) Holter recording was carried out in all participants of the study and then it was analyzed with BTL Cardiopoint software (Version 2.2; https://www.btl.co.id/produk-kardiologi-software-kardiopulmonari). During the ECG monitoring patients had their normal daily activities, and they were making notes in the diary indicating the time of the specific activity. They were asked to go to bed at about 10 pm and get up in the morning at about 6 am PVC burden was calculated in three time intervals: morning (02:00–09:59), day (10:00–17:59), and night (18:00–01:59). The frequency- and time-domain heart rate variability (HRV) parameters were also calculated [11]. Standard deviation of normal R-R intervals (SDNN) and standard deviation of the average normal-to-normal intervals calculated over 5-minute intervals (SDANN) represent global ANS activity. Root mean square of successive R-R interval differences (RMSSD), percentage of normal R-R intervals that differ by 50 ms (PNN50), and high frequency (HF) power represent parasympathetic nervous system activity. Low frequency (LF) power represents sympathetic nervous system activity. LF/HF ratio represents balance between sympathetic nervous system and parasympathetic nervous system activity.
Saliva collection and biomarker assays
Saliva samples were obtained with 5 mL cryovial tubes. All frozen saliva samples were thawed, vortexed, and centrifuged at 1,500×g for 20 min at 2°C–8°C temperature. Samples were analyzed with a competitive immunoassay specifically validated for the quantitative measurement of salivary cortisol (Salimetrics LLC, State College, PA, USA) and salivary norepinephrine (Elabscience Biotechnology, Houston, TX, USA) according to the manufacturer’s instructions. Cross-reactivity of the anti-cortisol antibody with other relevant steroids was 0.16% (11-deoxycortisol), 0.13% (cortisone), 0.21% (corticosterone), 0.01% (progesterone), and <0.01% (testosterone, aldosterone, estradiol). Intra- and interassay variances for cortisol measurement were 4.6% and 6%, respectively; and for norepinephrine measurement were 5.5% and 6.1%, respectively. For circadian rhythm level during the morning, day, and evening time, salivary cortisol and norepinephrine levels were obtained at the three collection times (6–7 am, 10–11 am, and 10–11 pm). By measuring thrice a day, we intended to observe the pattern of high to low levels of cortisol and norepinephrine at day and night in PVC patients.
Psychological questionnaires
Stress levels were measured using the Indonesian version of the PSS-10 questionnaire [11]. This rating scale measures the perception of psychological stress during the last month, and reports on situations of daily life that are considered as stressful. Also, it explores the level of stress experienced over the last month on a 5-point scale (0=never, 1=almost never, 2=once in a while, 3=often, 4=very often). Six of the 10 items are worded and scored in the non-reversed direction (i.e., “How often have you felt that you were unable to control the important things in your life”). Four of the 10 items are worded and scored in the reversed direction (i.e., “How often have you felt that things were going your way”). The scale is easily understandable by the general population, independent of education level. The scale total score ranges from 0 to 40. Scores ranging from 0–13 would be considered as low selfperceived stress. Scores ranging from 14–26 would be considered as moderate self-perceived stress. Finally, scores ranging from 27–40 would be considered as high self-perceived stress.
Self-rated health scale is a measurement of which a person believes or feels that his health is in good condition with a scale of 1 to 10, filled out during outpatient visits and at home in a diary format. The distance from the left edge of the line to the mark placed by the patient was measured to the nearest scale and used in the analysis as the score of the patient’s self-rated health scale.
Statistical analysis
Quantitative baseline characteristics data were presented as mean±SD and compared among fast-, slow-, and independenttype groups using one-way analysis of variance (ANOVA). Categorical data were expressed as number and compared among groups using chi-squared tests. Repeated measures ANOVA was used to test differences in circadian rhythm of cortisol, norepinephrine, HRV, and self-rated health scale between fast-, slow-, and independent-type PVC subjects with Games-Howell posthoc test. Hypertension has previously been observed as one of prevalent comorbidities in PVC patients [12], and since hypertension proportion was not equally distributed among groups, analysis of covariance (ANCOVA) including hypertension as covariate was performed. Data from the control subjects as the benchmark references were included in tables and figures, but they were not included in statistical analysis. Analysis of the correlation between circadian rhythms of cortisol, norepinephrine, HRV, and self-rated health scale with circadian rhythms of PVC burden in fast-, slow-, and independent-type PVC subjects were performed using repeated measures correlation test. Variables that have significant correlation with the circadian rhythm of PVC burden are included in the linear regression analysis. To detect the existence and level of multicollinearity in the final model, tolerance and various inflation factors (VIF) were calculated. Outliers are identified using Cook’s distance.
RESULTS
Characteristics of the study population
A total of 100 patients were approached to participate in the study (Figure 1). Five patients declined salivary sample collection. Five patients were excluded because they had a cold. Five patients refused to participate in the research because they prioritized time for personal family matters. Five patients refused to temporarily stop antiarrhythmic drugs. Five patients refused to participate due to favor of catheter ablation. Five patients refused due to occupied work schedule. Five patients refused to participate in the research because they no longer had any symptoms. Eventually, a total of 23 fast-type (mean PVC burden±SD=15.7%± 7.1%), 20 slow-type (8.5%±2.4%), and 22 independent-type (13.6%± 5.1%) PVC subjects were included in this study. The sociodemographic characteristics of fast-, slow-, and independent-type PVC are listed in Table 1. Independent-type PVC subjects had a significantly lower proportion of hypertension.

Flow chart of the study. PVC, premature ventricular contraction.
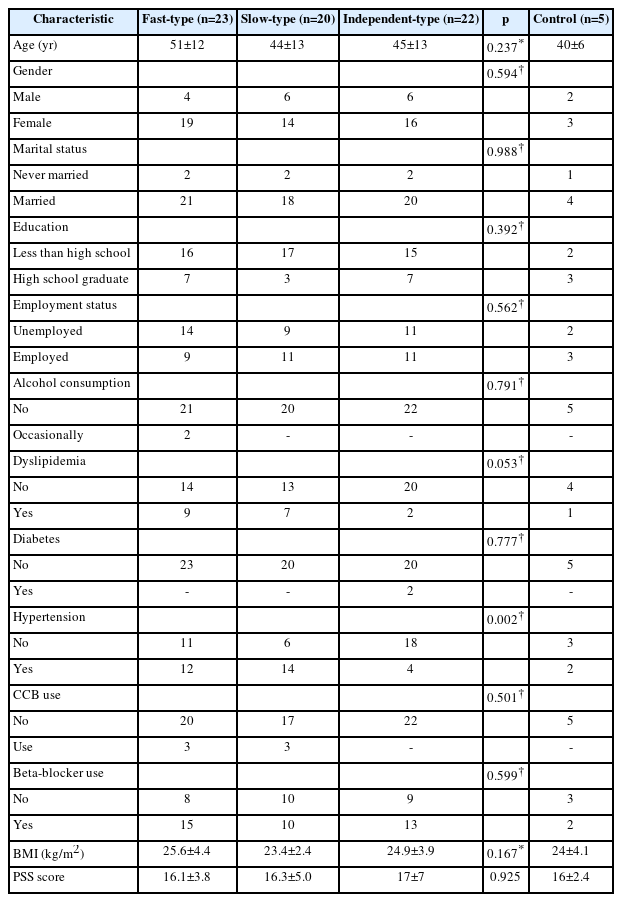
Sociodemographic characteristics of study participants
Circadian rhythms of heart rate and PVC burden
Heart rate and PVC burden circadian rhythm are presented in Figure 2 (Supplementary Table 1). Heart rate in independent-type PVC was higher than fast- and slow-type PVC. The gap is clear between heart rate of independent-type PVC and fast- or slowtype PVC, especially at night. Even so, the three groups had similar pattern of heart rate circadian rhythms, which was higher in the morning and lower at night.
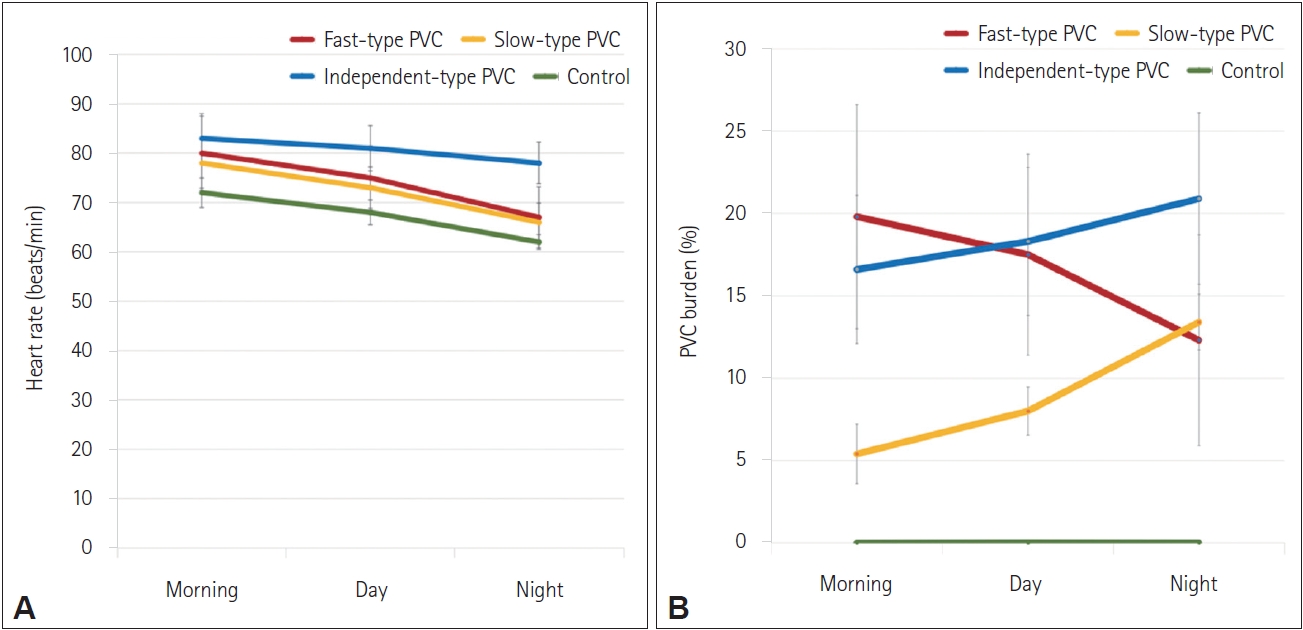
Circadian rhythm of heart rate (A) and PVC burden (B). PVC, premature ventricular contraction.
Circadian rhythms of cortisol and norepinephrine
The circadian rhythm of cortisol of the independent-type PVC was significantly different than that of other groups (fast-vs. independent-type and slow-vs. independent-type; p<0.05). In independent-type PVC, cortisol’s highest level was at night time. In fast-type PVC, cortisol level was higher in the morning and during the day compared to night time. In slow-type PVC, cortisol level was lower at night but higher in the morning. The norepinephrine level was highest in the morning in fast-type PVC, at night in slow-type PVC, and stayed consistently high throughout day and night in independent-type PVC, with significant intergroup differences (p<0.05) (Table 2). Hypertension was not statistically significant as covariate in ANCOVA, hence hypertension had no account for the results of cortisol and norepinephrine comparisons among groups.

Differences in cortisol, norepinephrine, HRV, and self-rated health of participants according to PVC circadian types
Circadian rhythms of HRV
In independent-type PVC, SDNN throughout day and night was lower compared to fast- and slow-type PVC (p<0.05). Additionally, parasympathetic nervous system activity was predominantly higher in the nighttime in fast- and slow-type PVC, while parasympathetic nervous system activity was lower in independent-type PVC throughout day and night with a significant difference (p<0.05). There were no significant intergroup differences in LF:HF ratio. However, compared to fast- and slow-type PVC, LF:HF ratio in independent-type PVC tends to be lower in the morning than at night (Table 2). Hypertension was not statistically significant as covariate in ANCOVA, hence hypertension had no account for the results of HRV parameters’ comparisons among groups.
Association between parameters and PVC burden
In fast-type PVC, repeated measures correlation test showed that there was a positive correlation between PVC burden and cortisol (Table 3). It also showed a negative correlation between PVC burden and parasympathetic nervous system activity (pNN50 and RMSSD). In slow-type PVC, PVC burden had negative correlation with cortisol and LF:HF ratio; while having positive correlation with norepinephrine, SDNN, RMSSD, pNN50, and HF. In independent-type PVC, PVC burden had positive correlation with cortisol and LF:HF ratio; and negative correlation with selfrated health scale.

Association between cortisol, norepinephrine, HRV, and self-rated health with PVC burden
Table 4 shows the multiple linear regression analysis of circadian related factors associated with PVC burden. In fast-type PVC, multiple linear regression showed that high burden of fasttype idiopathic PVC was associated with higher cortisol levels and lower parasympathetic nervous system tone. SDNN and RMMSD variables had a VIF of more than 10 so they were excluded from the linear regression analysis. VIF value more than 1 indicates that the independent variable is influenced by collinearity and although there are no definite rules, the VIF value more than 10 is interpreted as an indicator that the correlation (collinearity) between the independent variables is very high so that the standard error of the regression coefficient is too high and the estimated regression coefficient tends to be rough.
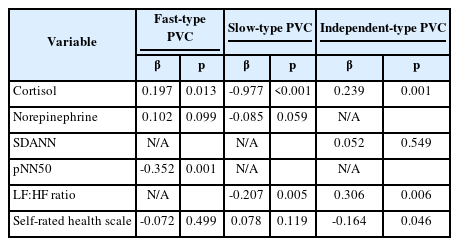
Multiple linear regression analysis perfomed between cortisol, norepinephrine, HRV, and self-rated health with PVC burden
In slow-type PVC, the high burden of slow-type idiopathic PVC was associated with lower cortisol levels and lower sympathetic nervous system tone. SDNN, RMMSD, pNN50, LF, and HF variables have a VIF of more than 10 so they were excluded from the linear regression analysis. In independent-type idiopathic PVC, the high burden was associated with higher cortisol levels and sympathetic nervous system tone as well as lower selfrated health scales. Norepinephrine and SDNN had a VIF of more than 10 so they were excluded from the linear regression analysis.
DISCUSSION
The present study describes novel knowledge regarding the factors associated with circadian rhythms of idiopathic PVC burden (Figure 3). Cortisol was positively correlated with fast- and independent-type PVC burden; and negatively correlated with slow-type PVC burden. Meanwhile, norepinephrine was not correlated with PVC burden circadian rhythm. Parasympathetic nervous system activity was negatively correlated with fast-type PVC burden. Sympathetic nervous system activity was negatively correlated with slow-type and positively correlated with independent-type PVC burden. Self-rated health scale was negatively correlated with independent-type PVC burden. It could be useful to understand the circadian rhythm type when managing idiopathic PVC patients because their psycho-neuro-endocrine characteristics are different.
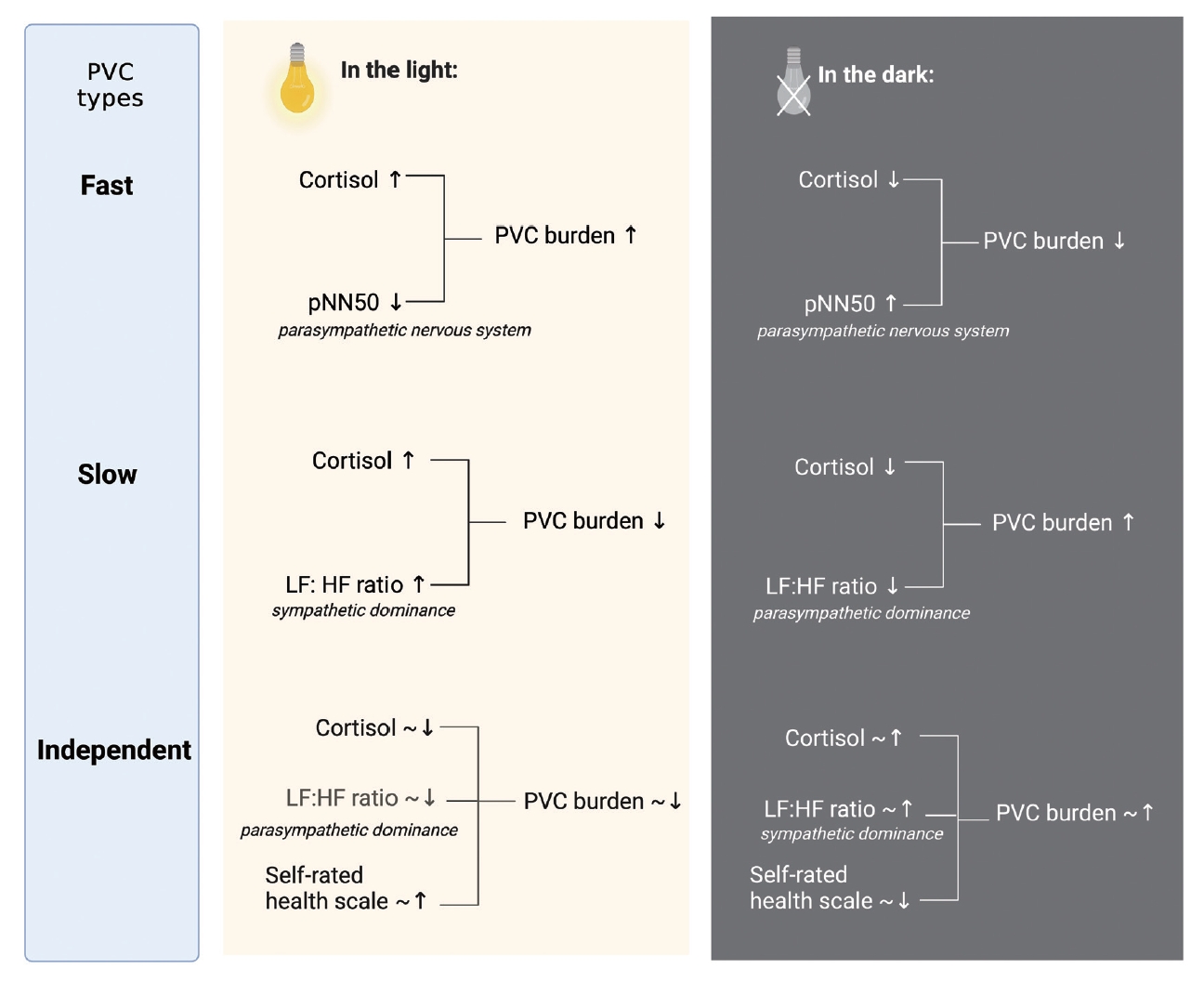
Proposed model of PVC burden circadian rhythm. PVC, premature ventricular contraction; pNN50, percentage of normal R-R intervals that differ by 50 ms; HF, high frequency; LF, low frequency.
In fast-type PVC, cortisol levels were lower and parasympathetic nervous system activity was higher in the evening which correlated with lower PVC burden. Meanwhile, in the morning and during the day, cortisol levels were higher and parasympathetic nervous system activity was lower, which correlated with higher PVC burden. The cortisol circadian rhythm in fast-type PVC is typical of the control subjects, but with higher cortisol levels throughout the day. Previous studies stated that the fast-type’s PVC burden is positively associated with the sympathetic nervous system [13]. In relation to the sympathetic nervous system, this study found norepinephrine levels increased in the morning than during the day and in the evening in fast-type PVC. Therefore, the increase in cortisol levels in the morning can be caused by an increase of sympathetic tone which is related to the increase in the morning PVC burden in fast-type PVC.
In slow-type PVC, lower cortisol levels and lower sympathetic nervous system activity in the evening correlated with higher PVC burden. Whereas during the day, cortisol levels were higher and the activity of the sympathetic nervous system was higher which correlated with lower PVC burden. This circadian rhythm of cortisol is inversely proportional to the slow-type PVC burden circadian rhythm where PVC burden was the lowest in the morning and the highest in the evening. Previous studies have shown that PVC can also be caused by the mechanism of early afterdepolarization (EAD) due to triggered activity [14]. Fast heart rate inhibits EAD and slow heart rate facilitates EAD so it is possible that slow-type PVC is related to EAD which is facilitated by increased tone of the parasympathetic nervous system accompanied by a slow heart rate. Night-time PVC may thus be both distressing and harmful. But how can it be ameliorated? Besides treatments, environmental factors (intrusive sound/light exposure) may be contributing and should be modified. Generation of a normal circadian sleep-wake pattern depends upon exposure to diurnal patterns of environmental sound and light, loss of which may thus worsen sleep patterns. Further studies are needed to investigate the use of conservative techniques to improve sound and light exposure and their impact on slow-type PVC burden.
In independent-type PVC, lower cortisol level and sympathetic nervous system activity during the day as well as higher selfrated health scale correlated with a slightly lower PVC burden. However, in the evening, cortisol levels and sympathetic nervous system activity were slightly higher, while self-rated health scale was slightly lower which correlated with slightly higher PVC burden. Furthermore, in the morning, during the day, and in the evening, the overall function of autonomic nervous system which was characterized by SDNN and the parasympathetic and sympathetic tones which were characterized by RMSSD, pNN50, LF, and HF in independent-type PVC were lower than those of fastand slow-type PVC. Previous studies have shown that a lower HRV is associated with a 32%–45% increased risk of a first cardiovascular event in patients without known cardiovascular disease [15]. In addition, a low SDNN is associated with a left ventricular ejection fraction (LVEF) of <35% where the relative risk is 6.7 compared to patients with LVEF above 35% [16]. This is in line with previous studies where consistency of PVC burden throughout the day in independent-type PVC was a predictor of decreased LVEF with an odds ratio of 16.3 [17]. Therefore, due to these results and worse prognosis of independent-type PVC, a study is needed to test whether a strategy of early rhythm-control therapy that includes PVC ablation would be associated with better outcomes in patients with independent-type PVC than initial medical therapy.
The present results show that fast-, slow-, and independenttype PVC patients have moderate perceived stress. They are in line with a report which appraised the psychological distress in cardiovascular patients [18]. Possible arguments may be brought in: knowing one has cardiovascular disease is triggering, let alone having responsibility to understand and choose treatment, financials, or family issues. Further studies are needed to investigate the triggers of perceived stress in PVC patients and if there is a need for additional education on health-related issues.
This study was the first to investigate HPA axis, autonomic nervous system, and self-rated health in premature ventricular complex, specifically based on circadian types. Data collection with Holter and saliva was non-invasive thereby minimizing pain and discomfort compared to venipuncture procedures which can affect heart rate and HRV and induce a cortisol response with a probability of around 30% [19,20]. However, because this study is observational in nature, there may be residual confounders. Also, this study protocol was used to observe an associative relationship, but not a causal one, between the burden of PVC and circadian factors.
In conclusion, higher cortisol levels and lower parasympathetic nervous system tone are associated with higher burden of fasttype idiopathic PVC. Lower cortisol levels and lower sympathetic nervous system tone are associated with higher burden of slowtype idiopathic PVC. Higher cortisol levels and sympathetic nervous system tone as well as lower self-rated health scales are associated with higher burden of independent-type idiopathic PVC.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.33069/cim.2023.0017.
Circadian rhythm of heart rate and PVC burden
Notes
Funding Statement
None
The authors have no potential conflicts of interest to disclose.
Availability of Data and Material
The data will be available for the readers if requested for further PVC circadian rhythm research.
Author Contributions
Conceptualization: all authors. Data curation: Novita Gemalasari Liman, Sunu Budhi Raharjo, Bambang Budi Siswanto. Formal analysis: Novita Gemalasari Liman, Sunu Budhi Raharjo, Joedo Prihartono, Bambang Budi Siswanto. Investigation: Novita Gemalasari Liman, Sunu Budhi Raharjo, Ina Susianti Timan, Bambang Budi Siswanto. Methodology: Novita Gemalasari Liman, Sunu Budhi Raharjo, Ina Susianti Timan, Bambang Budi Siswanto. Project administration: Novita Gemalasari Liman, Sunu Budhi Raharjo, Bambang Budi Siswanto. Resources: all authors. Software: Novita Gemalasari Liman, Sunu Budhi Raharjo, Bambang Budi Siswanto. Supervision: all authors. Validation: all authors. Visualization: all authors. Writing—original draft: Novita Gemalasari Liman. Writing—review & editing: all authors.